| © 2010 Dr Jan Polak |
| What is BMT ? |
|
Please scoll the window
What is the basic principle ? For BMT, aching joints (spinal or peripheral) and mobility restrictions are almost always due to muscle spasms, i.e. abnormal involuntary lasting contractions of muscles crossing the joint. This is confirmed by the practice : if musculoskeletal contractures are always found on clinical examination, and if by treating only those spasms the pain disappears and mobility is recovered, then the cause can only be muscular. With BMT these spasms will be treated by shortening the concerned muscles, instead of stretching them as is usually done. We will explain here the reasons why. What are the cause and the consequences Skeletal muscles account for about half the mass of the body. These muscles have several roles : they not only create the movements, but also maintain postures and positions ; furthermore they allow joint coaptation, and they protect joints against dislocation in case of shock. The main reflex that governs the skeletal muscles is the stretch reflex, which causes every stretched muscle to contract to recover its original length. This reflex helps to maintain positions and postures against gravity, which tends to change them, thus stretching the muscles that oppose this change : as soon as they are stretched, they return to their original length. This also allows some automatic reflex movements such as walking ; it avoids decoaptation, and it is this reflex again that protects joints in case of trauma. For the intensity of the contraction caused by the stretch reflex depends on the speed and/or amplitude of the muscle stretch. In other words, the more sudden and/or important the stretch is, the stronger the contraction reflex will be. The shortening stops by itself once the muscle is shortened, thus no longer stretched. What happens in case of trauma ? The muscles on the side from which the shock comes are suddenly stretched. This causes a reflex contraction proportional to the intensity of the shock, in order to protect the joint. But if this shock was intense, we often find that the contraction of the muscles involved does not stop any more : a spasm, a contracture was created (we will return later on the details of its mechanism). And this contracture will have no tendency to stop by itself, so that one will find it identical weeks, months and years after the shock. On examination, a contracture is in fact easy to diagnose : patient lying, the palpated muscle is hard and painful. So it is simple to ascertain the presence or absence of a contracture. One can sometimes find joint deformity in the direction of muscle contraction : the spasmed muscle is shortened, since contracture is an involuntary reflex contraction persisting indefinitely, a ß loop as we will see. There is also a limitation to the range of any passive movement that stretches the spasmed muscle, movement that can quickly become painful. Last, the active contraction of the contractured muscle is painful. The muscle crossing the joint it governs, these latter two elements make the patient feel the pain in the joints, and they limit their movements.
Results of a physical shock Diseases caused by lasting contractures The post-traumatic persistent skeletal muscle spasms (contractures) that we have just described will not be without consequences. The first one is pain, that will occur primarily during movements, but also often spontaneously. It can be felt at the muscular body (thus apparently at the joint crossed by the muscle), or at the tendon, that is its extension (= tendinitis), or at the tendon's insertion on the periosteum (= enthesopathy, like in epicondylalgia). Pain and/or muscle stiffness restrict movements. Since the spasmed muscle is hard and expanded at its center, it may compress nerves, blood vessels or viscera situated against it, causing neuralgia, venous disorders, vertigo, migraine, headaches & and visceral disorders of all kinds. Since the skeletal muscles represent half the mass of the body, one can suspect that the diseases due to contractures will be very numerous. Osteoarthritis is of no consequence at all Osteoarthritis is not responsible for any symptom (see also <http://osteoarthritis.bmt.free.fr>). It is a radiological image simply showing bone remodeling, as a reaction to the destruction of articular cartilage. Where do cartilage destruction and the ensuing osteoarthritis come from ? Apparently from persistent muscle spasms (contractures) that limit mobility of the joint and compresses it. Experience in animals (Akeson : The effects of immobilization on joints; Clin. Orthop. 1987) has shown that the immobilization and compression of a joint leads to : 1) destruction of articular cartilage, and 2) a bone remodeling reaction with all the x-ray symptoms of osteoarthritis. The speed of the process depends on the importance of both immobilization and compression. In the case of contractures it will take several months. Confirmation of this theory is that clinical symptoms classically attributed to osteoarthritis (pain, restriction of movement) disappear by healing the local muscle contractures, always present before treatment by BMT in case of osteoarthritis, and absent after it. Yet osteoarthritis itself persists after BMT, identical on x-rays, but totally asymptomatic : osteoarthritis was thus not responsible for any pain, but rather a consequence of that which also causes pain : post-traumatic persistent contractures (which may manifest clinically years after the initial trauma, following a triggering factor which should not be taken for the cause). Since the process of osteoarthritis takes some time, its importance simply gives an idea of the duration of the post-traumatic contractures.
The mechanism of Osteoarthritis Why care about muscles and not about bones ? The use of the word osteopathy leads to confusion. Bone is not the cause of any symptom (except in cases of fracture), and so even in cases of osteoarthritis, as we have seen, and 'displaced' bones do simply not exist. Vertebrae can however not be exactly in the right place. But this is not the cause of a symptom. Bone is a living but totally inert substance, like a rubber that you hold in your hand : a bone does not move unless muscles do move it, and it remains in place if muscles hold it there. Otherwise, it would drop, since bones like rubbers are subjected to gravity. Bones are just an inert frame that does not move neither stay in place without the action of the muscles. A demonstration skeleton is held together only by strings and a support, otherwise it would fall into pieces. And one can try to block two bones of a skeleton together, it will not be possible, since they are shaped as to allow smooth movements : one part of the one convex and the other concave. So if a bone is slightly out of place, or even blocked (which is rather rare, apart from changes in the cervical curve), only muscles can keep them so. And for the problem to persist, the concerned muscles have to contract continuously, which means that they are spasmed. And as for osteoarthritis, it is the contracture, spontaneously persistent, but reversible with specific treatment, ideally Brachy-Myotherapy, which is the cause of the symptoms, and the only purpose of treatment. Addressing the problem through the bone is impossible and leads necessarily to deal in fact with the contractured muscles - even without knowing it -, but in a complicated way, which will inevitably be less effective than if it was handled directly by BMT. Contracture, once installed, has no spontaneous tendency to heal, unlike what is sometimes written in medical literature : it only takes examining a patient to see that such untreated muscle dysfunction persists for months and years, in fact forever. However, as this is only a self-sustaining reflex loop (as we shall explain further on), simply to cut this reflex is enough to stop the spasm, and so the symptoms due to it. That is specifically done with BMT. With this simple approach, disorders of the musculoskeletal system (i.e. joint and myofascial pain, and joint range restriction) which otherwise persist with no tendency to improve, will on the contrary be fairly simple to cure. In short, contractures, causes many diseases, are spontaneously irreversible, but reversible with a specific treatment.
How does BMT work ? It is a simple technique, using the same method to treat each and any affected muscle, since the mechanism of contracture is unique, and because the only cause of joint pain and movement restrictions is always and only a persistent post-traumatic muscle spasm, called contracture. To stop the self-sustained reflex loop (or ß loop), which maintains the spasm, BMT will act by putting the corresponding joint in a position that shortens the contactured muscle - and not by stretching it as is usually done. Stretching a muscle causes a stretch reflex, that will induce more contraction, worsening the permanent involuntary contraction that the contracture is. Hence the name of the method : Brachy-Myotherapy, from the Greek words bracÚj brachy = short, myo = muscle, and therapy = treatment : the contractured muscle is shortened, and the treatment is made by shortening it even more ... This is done by a simple but precise protocol (details cannot be explained here, this being a simple presentation of the method). Other important factors contribute to the originality of the BMT, apart from shortening the contractured muscles as sole treatment.
Two other specificities of BMT The two most important ones are: 1) The primary cause of the symptoms the patient feels is usually elsewhere in his body. In practice, and this has never been shown to be wrong, only the muscles of the neck or the ankles can primarily be contractured after a shock. These are actually two parts of the body where the muscles are working constantly as soon as one sits (neck) or stands (neck & ankles). There is thus much strain put on them, and so they are easily overworked and weakened, whereas the other muscles contract occasionally. But we said that one can observe that all the joint pains are caused by contractures. In practice, the body seems somehow to spread the primary cervical or ankle contracture randomly throughout the body, by the means of different mechanisms, as to relieve the primary site, causing a latent increase of tone of most muscles of the body, which will manifests clinically at a given place in response to a trigger - which only increases the already abnormally high tone, compensating the primary neck or ankle contractures. It is important not to mistake the trigger for the cause unfortunately this is usually done...
A primary post-traumatic neck contracture, and its compensations Possible triggers are numerous, and since they are too often mistaken for the cause, this results in failure of treatment or relapses : actually the only real cause is to be found in post-traumatic contractures of the neck or ankle (recent or old, and often asymptomatic, since well compensated). To treat them is always necessary, and often sufficient. It is common not even to deal with the painful area itself, precisely to cure it - it is only a decompensated compensation, which has no more raison d'être when the primary trouble is treated ! The choice between neck or ankle as the primary site is made by examination. 2) The second important originality of Brachy-Myotherapy is based on the fact that there are two kinds of skeletal muscle fibers : ¤ type I fibers, with lasting contraction after a slight startup latency ; ¤ type II fibers, whose contraction is fast but short in duration. In practice all the skeletal muscles are composed primarily of one or the other kind of fiber (which corresponds roughly to the distinction between dark and light muscles). A muscle has therefore a function of joint mobilization, of creating movement, when it contains mostly type II fibers - these muscles are called dynamic ; or its function will be to hold a position or posture, when it consists mainly of type I fibers - these muscles are called tonic. What matters is that only the tonic muscles can be spasmed, contractured. This can never be the case for dynamic muscles, because the neurological system governing type II muscle fibers contains circuit-breakers (Renshaw cells) to prevent a prolonged contraction, that nervous systems governing muscle toning have not. Now in the body there are about as many muscles that create movement as there are muscles that hold the positions thus obtained. So only more or less half of the muscles of the body can be contractured and cause various symptoms like joint pain or movement restrictions, and thus only these muscles have to be treated. We were able to establish a precise list of tonic muscles, particularly through clinical observation, because as far as we know such a classification of muscles did not yet exist. This distinction can help to better target the treatment.
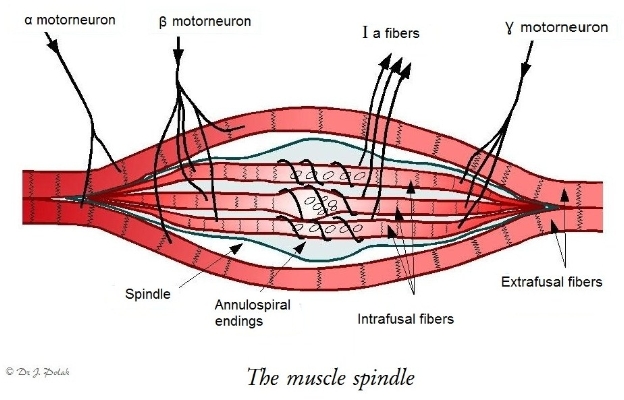
What is the cause of a contracture ? To understand this, a short reminder of some other basic notions of muscle physiology is necessary. A skeletal muscle, whether tonic or dynamic, is composed of two kinds of muscle fibers. It is of course mainly made of fibers that allow its shortening. These fibers, called extrafusal, are mainly stimulated by the alpha motor neurons (aMN) extending from the anterior horn of the spinal cord. But among the mass of these fibers are scattered special fibers, called intrafusal because they are walled off from the rest of the muscle by a collagen sheath that has a spindle shape. These fibers are structured in 3 parts : the two ends are contractile, whereas the core, from which annulospiral endings start, is sensitive to stretch. Acting as a mechanoreceptor, it is the origin of impulses responsible for the stretch reflex. When a muscle is stretched, the ensuing stretching of the central part of intrafusal fibers stimulates the Ia afferent fibers that have their origin there, and that will in turn stimulate the aMN of the anterior horn of the spinal cord. These will then stimulate the extrafusal muscle fibers, causing them to contract and thus shorten the muscle : this is the mechanism of the stretch reflex, cited earlier : any stretched muscle will contract.
This description is not quite complete. Actually the aMN do not innervate the muscle spindles ; but if one thinks about it, since it is their stretching that causes the stretch reflex, it is necessary that after the muscle stretch that has stretched them, they shorten as much as the muscle itself to be able to react to any new stretch. This is partly due to a mechanical dragging effect caused by the muscle shortening, sufficient for the spindle not to be stretched any more, and thus the stretch reflex to stop, but not enough to really give 'tension' to the intrafusal fibers, necessary for them to be fully responsive. Here the two contractile ends of the intrafusal fibers step in. They are innervated by beta motorneurons (ßMN), which are slightly different from the aMN. They originate also in the anterior horn of the spinal cord, and they innervate both contractile ends of the intrafusal fibers, as well as the 'classic' extrafusal fibers (so called because they are outside the muscle spindles). ßMN are skeleto-fusimotor, while aMN are only skeletomotor. The Ia fiber described above, starting from the muscle spindle, once stimulated by spindle stretch, will send impulses to both aMN and ßMN. So when the muscle contracts after stretching, the ends of the intrafusal fibers will also contract. The ßMN seem to do so as a brief adjustment that allows the restoration of correct tension in the muscle spindles. The more rapidly a muscle spindle is stretched, the more intense its stimulation of the motorneurons by the Ia fibers will be. How can contractures and their persistence be explained ? It can be observed clinically that contractures occur after a trauma. To put this finding in relation to what we have just seen, we must remember that a physical shock will almost always cause at least one muscle to be suddenly stretched. A stretch reflex will ensue, resulting almost instantly in a reflex contraction of the muscles involved, which will protect the joint against dislocation (much better than would the ligaments, which are too loose because they must allow normal joint movement). The intensity of the contraction caused by the stretch reflex depends on the speed of muscle stretching and on the amplitude of it : in other words, the more the shock is sudden and intense, the more important the reflex contraction will be, which is perfectly suited to the protection function. At a neuromuscular level this can in our opinion be explained as follows : the more the muscle stretch is sudden, the more rapidly the muscle spindles are stretched. And the faster the central part of the intrafusal fibers will send impulses by the Ia afferent fibers to the alpha and beta motorneurons. And the more these are stimulated, the more they will in turn stimulate the muscle fibers they control, namely the extrafusal fibers for the aMN and both the intrafusal and extrafusal fibers for the ßMN. What the aMN concerns this explains why the more rapid or intense stretching is, the more the reflex contraction is important. However for the ßMN, that are supposed to adjust the tension of the muscle spindles to the global muscle length, the more the distal contractile parts of the intrafusal fibers are stimulated, the more the central part will be stretched. Beyond a certain threshold of speed and importance of stretch it is no longer an adjustment that is being done, but a vicious circle that settles : the contractile parts strongly stretching the equatorial parts of the intrafusal fibers, these will send an important impulse to the motorneurons by the Ia fibers. So the ßMN will in turn significantly stimulate the contractile parts of the intrafusal fibers, which will again stretch the central part, and so on. A reflex loop was created, which also stimulates continuously extrafusal fibers, thus creating a permanent contraction of the muscle : this is the muscle spasm or contracture. Since the stretch reflex depends mainly on ßMN, and the contracture being simply a self-sustained stretch reflex, we call this underlying mechanism a 'ß loop'. This is a monosynaptic loop, remaining purely on the spine level, without involvement of the superior nervous system, i.e. the brain. Once there, the loop is self-sustaining, so it has no reason ever to stop spontaneously ; that is the reason why a contracture does not tend to stop spontaneously, and will be found (if one looks for it...) months and years after starting.
Mechanism of contracture, or ß loop (One should not confuse this reflex loop with the 'gamma loop'. In fact the loop described above has little to do with the gamma motor neurons (?MN) - which also innervate the contractile parts of the intrafusal fibers, but depend on the superior nervous system. We can simply notice that such ?MN are stimulated under psychological stress, and then increase the tone of the intrafusal muscle fibers, explaining why contractures and their symptoms are exacerbated in times of stress. How can the action of BMT explained ? Since the muscle spasm, or contracture, persists indefinitely because the central parts of the intrafusal fibers of the muscle spindles are constantly stretched by the contractile distal parts, thereby causing the continuous contraction of muscle fibers (ß loop), if one wants to stop this involuntary contraction the easiest way is to stop the stretching of the muscle spindles by shortening them mechanically (there are other more complex ways - but simplicity is an important factor for efficiency). This is very simply achieved by shortening the muscle. To do this we place the joint governed by the concerned muscle in a position where the maximum shortening of this muscle is achieved. So this is what we do in Brachy-Myotherapy (BMT) : after an accurate diagnosis of every muscle contracture, we will shorten the dysfunctional muscles a bit more than they already are, for a specific time and according to a precise protocol. Hence the name of Brachy-Myotherapy, brachy coming, as we have said, from the Greek word meaning 'short'. The no longer stretched muscle spindles immediately cease to stimulate the motor neurons, and the permanent contraction of contracture ceases immediately. It is just as simple and logical as that. However, this treatment will usually have to be repeated several times since there are many muscle spindles in one muscle, and it is difficult to normalize a contracture completely in one session when several antagonistic muscles are concerned, which is usually the case. A hypertonic muscle is not easy to stretch, making it difficult to shorten the opponent one completely. Each muscle will have to be treated in turn several times, so that in an average 4-6 sessions all contractures will be processed. Conclusion : so what is BMT ? BMT (Brachy-Myotherapy) is probably the simplest of manual therapies - and perhaps also the most effective according to various studies. It is simple to apply, it can be learned quickly, and can immediately be but into practice with success. Its purpose is to deal specifically and directly with muscle contractures, which in practice are the cause of almost all joint pains and/or movement restrictions (whether there is osteoarthritis or not) - contractures that are also the cause of various visceral or venous disorders, neuralgias, sciaticas, migraines and other headaches. Bones can never be held for responsible since they are completely passive, moved as well as held in place only by the muscles. The primary cause of contractures (i.e. permanent involuntary contractions, even at rest) is traumatic, even if they may become manifested only after a non traumatic trigger factor. They have no tendency to stop in time, except by a specific treatment manual like BMT. Three things make the specificity our method : 1) The treatment of muscle contracture is done by passive shortening of the concerned muscle ; 2) The root cause of all diseases caused by contractures is to be found at the muscles of the neck or the ankles; 3) muscles used to make movements should be distinguished from those used to maintain positions or postures, since only the latter can have contractures. BMT is simple to learn and to apply, and can be taught to health care professionals in a short time, since there is no need to complicate what is simple - although update and rehearsal courses are highly recommended, because simple does not mean simplistic : BMT must be performed in a precise and rigorous way, and it is recommended that it be checked regularly every 2 or 3 years that mistakes have not crept into the practice. However basic training is immediately applicable, and BMT students will be immediately efficient after the first training course. © Dr. Jan Polak, MD Health care professionals who would like to receive more information |





 |
